

Page 2
Go to: Diagnosis, Confirmatory Testing, Discussion, Pathology Summary
Diagnosis
Peroxisomal biogenesis disorder/Zellweger Spectrum Disorder (PBD/ZSD)
Go to: Diagnosis, Confirmatory Testing, Discussion, Pathology Summary
Confirmatory Testing
- Plasma VLCFA analyses: consistent with a defect in peroxisomal fatty acid oxidation
- Abnormal accumulation of very long chain fatty acids (VLCFA) and phytanic acid
- Mutation analysis:
- Compound heterozygous mutations in the PEX26 gene (c.192_216del/c.353C>G: p. Prol118Arg)
Go to: Diagnosis, Confirmatory Testing, Discussion, Pathology Summary
Discussion
Epidemiology
- 1/50,000–100,000births in the US
Etiology/Pathogenesis
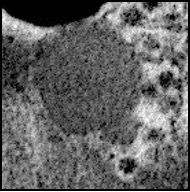
- PBD/ZSD is characterized by impaired peroxisomal functions and lack of peroxisomes confirmed by EM.
- What is peroxisome?
- Spherical, single membrane-bound, intracytoplasmic organelles
- 0.2–1 μm in diameter.
- Contains >50 enzymes contributing to multiple catabolic and synthetic biochemical mechanisms.
Genetic alterations
- Caused by mutations in the 14 known PEX genes [PEX1, PEX2, PXMP3 [PEX2], PEX3, PEX5, PEX6, PEX10, PEX11ts PEX12, PEX13, PEX14, PEX16, PEX19, and PEX26]
- Encoding peroxins (essential proteins required for normal peroxisome assembly)
- Mutations in PEX1 account for 58.9% of ZSD followed by PEX6 (15.9%), PEX12 (7.1%), PEX10 (4.2%), and PEX26 (4.2%).
Clinical Presentations
- ZSD were traditionally classified based on their clinical and biochemical features into the following diseases:
- Severe phenotype (Zellweger syndrome)
- Intermediate phenotype (neonatal adrenoleukodystrophy: NALD)
- Mild phenotype (infantile Refsum disease: IRD)
- Now, considered to be a continuum of the same disorder
- Patients with the most severe phenotype (ZS) present as newborns with:
- Severe hypotonia, seizures, respiratory distress
- Characteristic craniofacial dysmorphism:
- Flattened face, broad nasal bridge, high forehead, large anterior frontal, hypertelorism, high arched palate, and micrognathia.
- Brain: polymicrogyria, pachygyria, and heterotopias
- Visual defects: cataracts, glaucoma, optic atrophy, pigmentary retinopathy
- Sensory deafness
- Milder phenotypes (NALD and IRD):
- Symptoms become more apparent later in life with more variable and milder forms.
- Normal Hepatocytes contain many peroxisomes:
- Liver involvement is common.
- Usually, within the first year of life
- Hepatomegaly, cholestasis, elevated transaminases, and liver dysfunction
- Renal cysts:
- Often found at birth, supports the diagnosis.
Management
- Management is based on the symptoms.
- Dietary interventions: restriction of metabolites that accumulate and replacement of ones that are deficient – not systematically studied.
- Oral bile acid therapy improved hepatobiliary function in several infants with ZS.
- Patients have also received docosahexaenoic acid (DHA) supplementation – with controversial clinical benefits.
- “Hepatocyte” transplantation, which improved biochemical parameters, but clinical improvement has not yet been reported.
Prognosis
- Most patients with ZS die within the first year of life, while patients with milder phenotypes may survive into the second decade.
Go to: Diagnosis, Confirmatory Testing, Discussion, Pathology Summary
Pathology Summary
Microscopic features:
- Nonspecific
Ultrastructural features:
- Young patients with milder phenotypes may undergo liver biopsy without suspicion of PBD
- EM can play an important role.
- Lack of peroxisomes is the main diagnostic ultrastructural feature of ZSD.
- Small bodies resembling incompletely developed peroxisomes (ghost peroxisomes) can also be found.
- Large lysosomes containing abnormal inclusions, “trilamellar inclusions”
- Two thin linear electron-dense layers and a thin lucent layer between them
- Initially thought to be only specific for IRD (milder phenotype).
- The inclusions are presumably accumulated abnormal metabolic products and appear more prominent later in life.
